Laureato in Medicina e Chirurgia presso l'Università di Catania,
specializzato in Ortopedia e Traumatologia presso l'Università di Bologna
(Istituto Rizzoli) e specializzato in Fisiatria presso l'Università di Trieste.
Laureato in Medicina e Chirurgia presso l'Università di Catania,
specializzato in Ortopedia e Traumatologia presso l'Università di Bologna
(Istituto Rizzoli) e specializzato in Fisiatria presso l'Università di Trieste.Dr. Mario Nicolosi Specialista in Ortopedia e Traumatologia Specialista in Fisiatria
Il trattamento delle fratture della testa dell'omero con
emiartroplastiche cementate e non. La nostra esperienza
Treatment of fractures of the humeral head by cemented and
cementless hemiarthroplasty. Our experience
Cappelli editore, Bologna 2005 Chir. Organi Mov., XC,
171-177, 2005
M. Nicolosi, R. Gambaretti, L. Broffoni -
Chirurgia della Spalla e del Gomito, Istituto Ortopedico
Galeazzi, Milano
Sommario
Sono stati controllati i pazienti sottoposti ad intervento di
emiartroplastica di spalla per frattura della testa dell' omero.
La revisione è stata condotta per un periodo esteso dal 1991
al giugno del 2001 utilizzando 2 diversi modelli protesici: la
protesi di Neer cementata e la protesi di Randelli non
cementata. è stato possibile rivedere 93 casi sui 148 pazienti
operati. La revisione della casistica ha permesso di evidenziare
l'importanza fondamentale della ricostruzione delle tuberosità e
della rieducazione. Si è anche notato come l'età del paziente e
la gravità della frattura non condizionino affatto il risultato.
Gli esami radiografici non hanno messo in luce fenomeni di
mobilizzazione degli impianti protesici. Si è assistito ad
erosioni della glenoide solo quando concomitavano due fattori:
la cattiva posizione della protesi e la ipomobilità della
spalla. Lo studio ha permesso di mettere in evidenza numerosi
elementi prognostici, sia favorevoli che avversi,
quantificandone l'importanza e la priorità.
Parole chiave: frattura omero
prossimale; emiartroplastica; spalla.
La terapia delle fratture della testa dell' omero con
emiartroplastica è un trattamento ancora in fase di completa
definizione. In questi ultimi anni si è assistito, dopo un
iniziale entusiasmo e ottimismo, ad una revisione critica con
successiva riduzione delle indicazioni1,2,3.
Lo scopo di questo lavoro è quello di portare un contributo
sull'argomento, ponendo l'attenzione, oltre che sui meri
risultati statistici, anche sui fattori prognostici che incidono
sull' esito del trattamento così da trarne indicazioni sia sulla
tecnica chirurgica che sulla opportunità dell' intervento.
Materiale e metodi
Lo studio interessa i pazienti operati dal gennaio 1991 sino a
tutto il giugno del 2001. Il follow-up è di 43,2 mesi con un
range che va dai 6 mesi ai 10,5 anni. Nel periodo di tempo
citato i pazienti sottoposti a intervento di protesizzazione
sono stati 148. L'inter vento è stato eseguito in media dopo 4,5
giorni (range 2-18) dalla frattura. AI momento della revisione
53 pazienti erano persi al controllo e 2 erano già deceduti per
altre ragioni. Abbiamo quindi potuto controllare 93 soggetti. Di
questi 74 erano femmine e 19 maschi. L'età media dei pazienti
era di 70,02 anni. Il soggetto più giovane aveva 48 anni e il
più anziano 91. La spalla destra era interessata 49 volte e 44
la sinistra. Abbiamo adoperato la classificazione di Neer3,4
secondo la quale 12 fratture erano del tipo a 2 frammenti, 28
fratture a 3 frammenti e 53 fratture a 4 frammenti. I primi casi
(25) sono stati operati adoperando le protesi cementate di Neer.
In seguito, (68 casi) è stata adoperata la protesi modulare non
cementata di Randelli. Per la valutazione dei risultati sono
stati adoperati sia il Constant score che il Simple Shoulder
Test. Il risultato medio del Constant score è stato di 62,40 (range
42 - 79), quello del S.S.T. è stato di 6,8 (range O - 12). Per
tutti i pazienti è stato owiamente eseguito anche un esame
radiografico che ci ha permesso di confrontare i dati clinici
con quelli delle immagini.
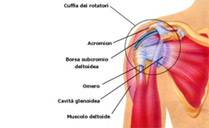
Tecnica chirurgica
I pazienti venivano posti nella posizione dell'astronauta. La
via chirurgica è stata solitamente quella di Larghi con accesso
all'articolazione attraverso la sezione del tendine del
sottoscapolare. Nei casi in cui era presente una grave
scomposizione delle tuberosità, con loro risalita e completo
distacco dalla diafisi omerale, l'accesso all'articolazione è
stato eseguito attraverso l'ampia breccia formatasi risparmiando
così il tendine del sottoscapolare. Si è proceduto poi
all'identificazione e all'isolamento delle tuberosità che sono
state affidate a fili di sutura non riassorbibili. La testa
omerale veniva quindi asportata e misurata per scegliere la
corrispondente testa protesica. Il tempo successivo è consistito
nella preparazione della diafisi omerale per effettuare
l'impianto dello stelo protesico. Prima di procedere
all'impianto definitivo è stato sempre eseguito un controllo
ampliscopico con la protesi di prova e con una ricostruzione
prowisoria e indicativa delle tuberosità. Un ulteriore controllo
radiografico, con relativa documentazione del risultato
ottenuto, è stato eseguito dopo l'impianto della protesi
definitiva e dopo l'accurata ricostruzione, con filo non
riassorbibile, delle tuberosità ottenuta sfruttando gli appositi
fori protesici e, alla bisogna, praticando dei fori sulla
diafisi omerale. Una cauta mobilizzazione passiva è stata sempre
iniziata il più presto possibile. L'immobilizzazione in tutore è
stata mantenuta per 4 settimane. Non sono mai state necessarie
trasfusioni ematiche.
Risultati
Il risultato medio del Constant Score è stato di 62,40 (range
42-79).
Per avere una valutazione più vicina alla realtà, avendo a che
fare con una casistica composta da pazienti con età media di 70
anni, bisogna tuttavia adoperare il Constant tipizzato secondo
le varie fasce di età (fig. 1).
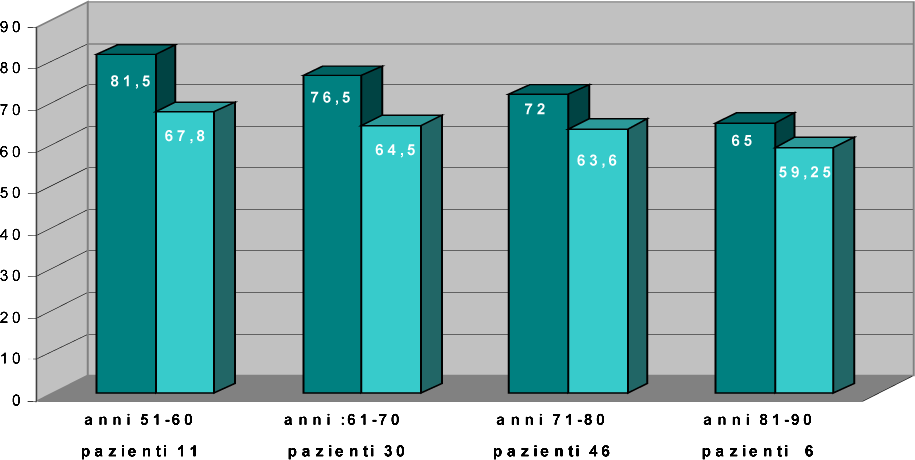
Fig. 1
Constant ponderèe per decadi.
Le colonne di colore più chiaro indicano i risultati ottenuti.
Analizzando i risultati per
fascia di età si vede, in realtà, come questi siano molto
più confortanti e rassicuranti dei primi. Abbiamo potuto
registrare, infatti, valori molto vicini percentualmente
al valore medio per fascia nella fascia di età che va dai
51 ai 60 anni (11 pazienti), 1'84,3% per i pazienti dai 61 ai 70 anni
(30 casi), 1'88,3%
nella fascia dai 71 agli 80 anni (46 pazienti) e il 91, 1 % per
quella dagli 81 ai 90 anni (6 pazienti). I 2 casi di 48 e di
91 anni sono stati collocati nelle fasce limitrofe per omogeneità
(non ci è sembrato opportuno creare ulteriori suddivisioni non significative
da un punto di vista statistico).
La media dei valori ottenuti per l'elevazione della spalla è
stata 112,6 gradi (i valori sono riassunti nella fig. 2).
I valori dell' extrarotazione e dell'intrarotazione sono esposti
in dettaglio nelle figg. 3 e 4.
Per quanto riguarda la forza i risultati sono riassunti nella
fig. 5.
I risultati ottenuti per quanto riguarda lo svolgimento delle
ATTIVITÀ quotidiane sono riassunte nella fig. 6.
I risultati ottenuti con il Simple Shoulder Test hanno
evidenziato un valore medio di 6,8 (range 0-12).
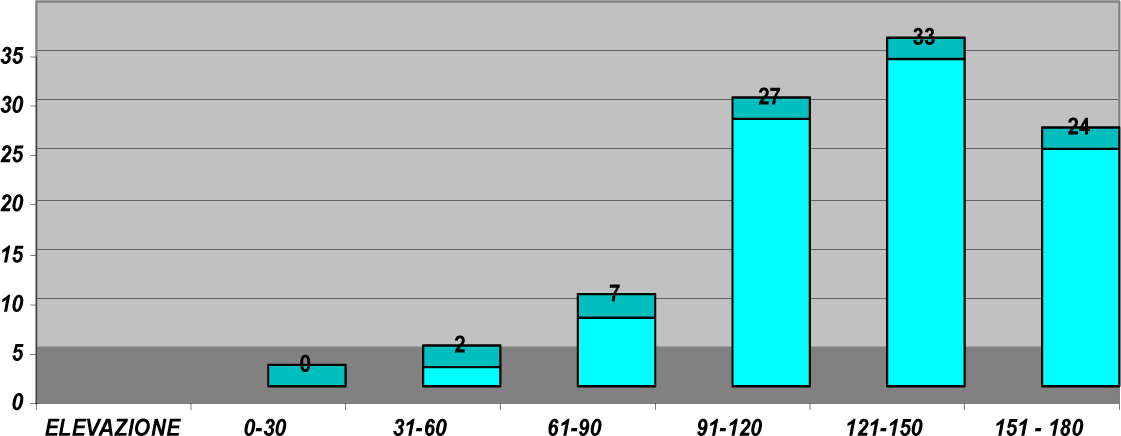
Fig. 2
Risultati concernenti l'elevazione.
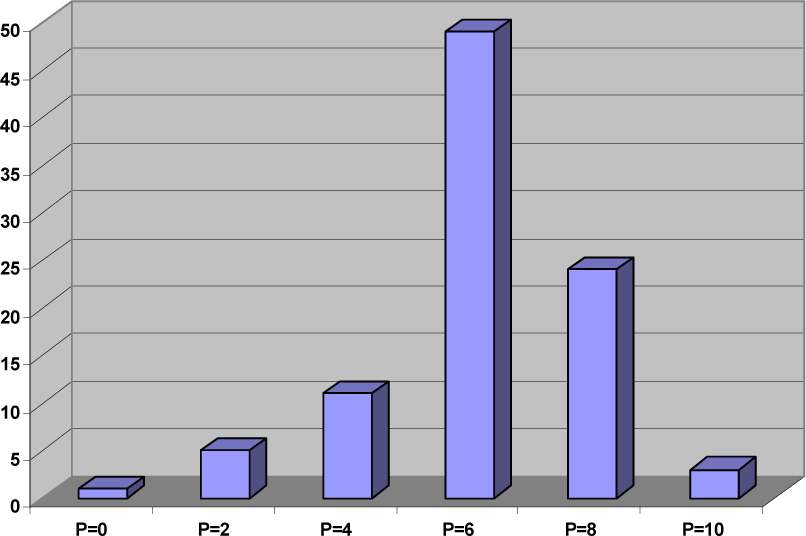
Fig. 3
Risultati concernenti l'extrarotazione.
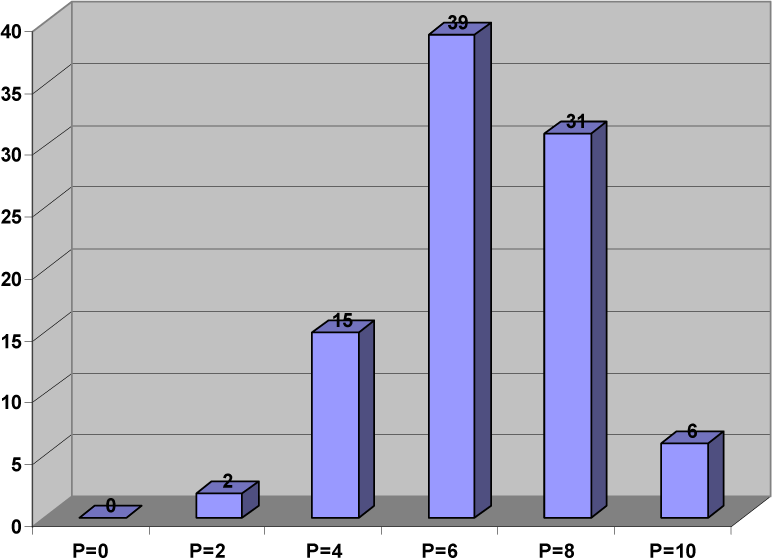
Fig. 4
Risultati concernenti l'intrarotazione.
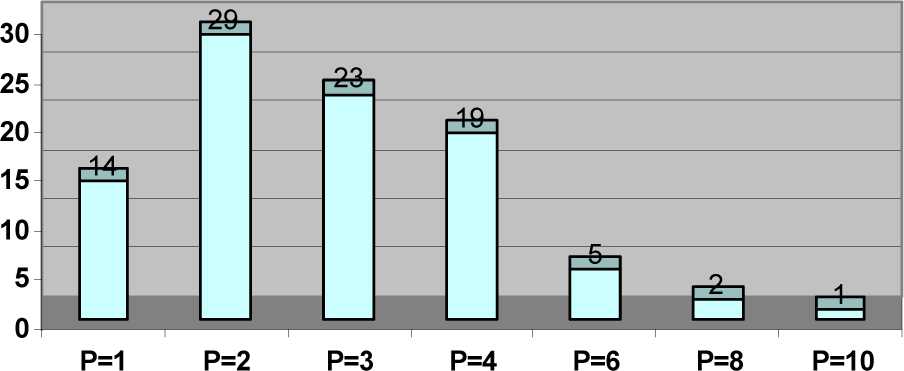
Fig. 5
Risultati concernenti la forza.
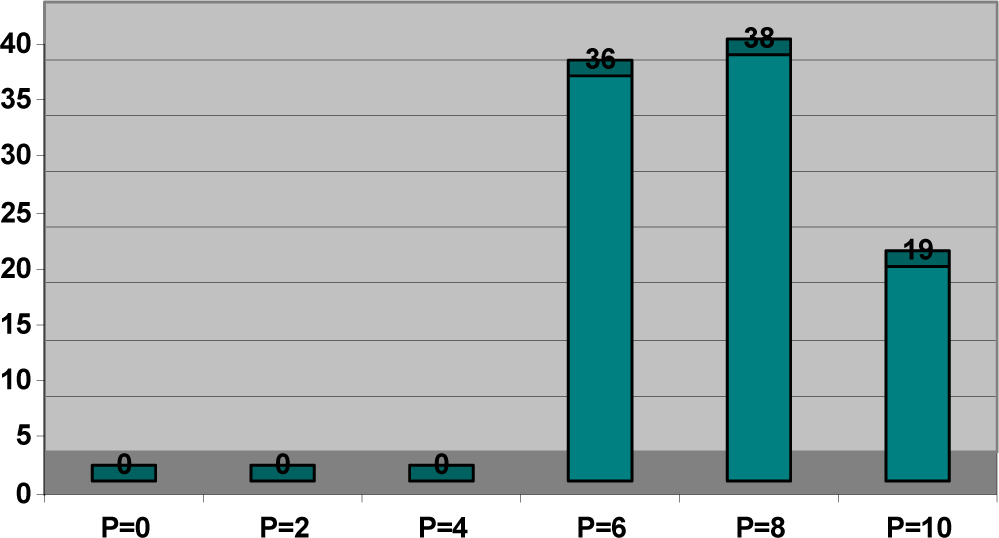
Fig. 6
Risultati concernenti le ATTIVITÀ quotidiane.
Discussione
La revisione della casistica è stata condotta con lo scopo
di valutare le variabili, sia anamnestiche che chirurgiche,
che contribuiscono al successo dell'intervento: età, sesso, tempo
trascorso tra il momento della frattura e l'intervento
chirurgico, via d'accesso, tipo di frattura, radiolucenza,
cementazione o meno dell'impianto, erosione della glena,
riabilitazione e motivazione dei pazienti.
Come si può chiaramente
notare dalla tabella della fig. 1, l'età non è un fattore prognostico
sfavorevole anzi, con il suo avanzare, il valore percentuale migliora. Ciò
è, naturalmente, dovuto al fatto che il valore medio del Constant ponderato
(tipizzato per fascia di età) si abbassa con l'aumentare
dell'età e quindi i buoni risultati sono più facilmente
raggiungibili oltre che più realistici. I risultati del Constant
tipizzato devono, a nostro awiso, servire a non ritenere che con
i pazienti più anziani si abbiano i risultati peggiori.
Neanche il sesso e il tempo trascorso tra il momento della
frattura e quello dell'intervento chirurgico sono stati elementi
prognostici che hanno influenzato il risultato finale. Nessuna
differenza è stata notata tra l'accesso articolare attraverso il
tendine del sottoscapolare o attraverso la breccia lasciata
dalla scomposizione delle tuberosità.
Un altro elemento prognostico che abbiamo preso in
considerazione è il tipo di frattura. Contrariamente a quello
che prima della nostra revisione pensavamo, abbiamo riscontrato
come il tipo di frattura non incida in modo significativo sul
risultato (fig. 7 e fig. 8).
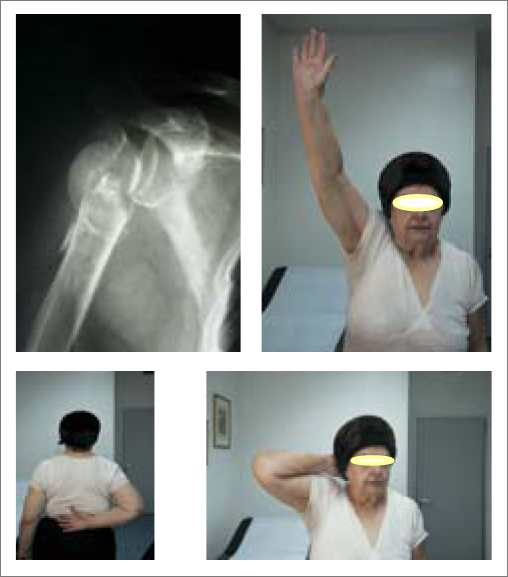
Fig. 7

Fig. 8
I risultati si sono distribuiti uniformemente tra i vari tipi di frattura a 2, 3 o 4 frammenti. Abbiamo, infatti notato, e più tardi torneremo sull'argomento, come anche una frattura a 2 frammenti, apparentemente semplice da affrontare chirurgicamente, possa esitare in risultati meno brillanti di una frattura a 4 frammenti, notevolmente scomposta, se non sono presenti canoni di una buona ricostruzione chirurgica o di una buona rieducazione funzionale. Un elemento prognostico che si è, invece, rivelato decisivo sul risultato finale è stato quello della ricostruzione delle tuberosità. è stata fatta molta attenzione alla posizione delle tuberosità durante 1'osservazione e il controllo delle radiografie. La sede rilevata è stata confrontata con i valori del Constant score: i migliori risultati globali sono sempre stati associati ad una corretta posizione delle tuberosità. Non solo: senza quest'ultima non si è mai avuto nessun risultato soddisfacente per quanto riguarda la motilità della spalla sia in elevazione che in extrarotazione come in intrarotazione (fig. 9).

Fig. 9
Le stesse complicazioni (importanti deficit di movimento senza per fortuna dolore) sono apparse quando abbiamo riscontrato il riassorbimento delle tuberosità. (fig. 10).

Fig. 10
Altro fattore
prognostico che abbiamo preso in considerazione è stata la
radiolucenza. Quest'ultima però non ha mai trovato
corrispondenza con la clinica. I pazienti, le cui radiografie
mostravano fenomeni di radiolucenza, non presentavano, infatti,
nessun segno clinico di dolore né spontaneo né durante il
movimento della spalla.
In nessun caso abbiamo riscontrato fenomeni di mobilizzazione
dell'impianto protesico sia cementato che non cementato (fig.
11).

Fig. 11
dopo 10,5 anni
Noi abbiamo adoperato sia impianti protesi ci cementati che
non. Nessuna differenza è stata costatata tra i due tipi
di protesi sia per quanto riguarda i dati radiografici che
quelli clinici.
Un altro elemento che abbiamo preso in considerazione è
l'erosione della glenoideo Nella nostra casistica è apparsa solo
3 volte. Ciò che abbiamo potuto costatare è che i' erosione
ossea si realizza solo in concomitanza di 2 fattori: la non
corretta posizione della testa protesica rispetto alla glenoide
e la scarsa motilità della spalla (figg. 12 e 13). Quando,
infatti, la sfericità della testa protesica non coincide con
la cavità glenoidea, la zona in cui si svolge il movimento tende a
restringersi. Quando a questa evenienza si associa anche la
scarsa motilità della spalla, le forze di attrito si concentrano
in una zona ancora più piccola e l'erosione ossea è inevitabile.
Nei casi in cui, invece, sia presente solo una cattiva posizione
della testa protesica rispetto alla glena o solo una scarsa
motilità della spalla, non abbiamo mai osservato erosione ossea
(figg. 14 e 15).
Ulteriore elemento di verifica è stata la rieducazione
funzionale della spalla. Non sempre e per tutti i pazienti
è stato possibile eseguire in maniera corretta la kinesiterapia.
I pazienti, spesso anziani e con notevoli difficoltà logistiche,
hanno, non raramente, eseguito pochi cicli di rieducazione:
in questi casi, nonostante un buon posizionamento dell'impianto, i
risultati per quanto riguarda la motilità della spalla ha dato
valori deludenti sebbene i pazienti non lamentassero dolore e
fossero soggettivamente contenti. Lo stesso si può dire per
quanto attiene alla motivazione dei pazienti. L'esecuzione
attenta, costante, puntigliosa, motivata degli esercizi di
rieducazione ha sempre premiato, mentre l'atteggiamento
contrario ha sempre prodotto scarsi risultati.
Per concludere, dunque, vogliamo ribadire come gli elementi
dai quali non si può prescindere per avere buoni risultati
dal trattamento protesico delle fratture dell'estremo prossimale
dell'omero siano l'accurata ricostruzione anatomica, con
particolare riguardo per le tuberosità, e la rieducazione
post-operatoria.

Fig. 12-13
Erosione della glena dovuta alla concomitanza di 2 fattori: cattiva posizione della protesi e scarsa motilità della spalla.

Fig. 14
Cattiva posizione della protesi ma buona motilità: nessuna erosione glenoidea.
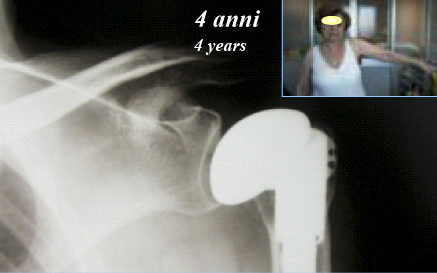
Fig. 15
Poca motilità ma buona posizione della protesi: nessuna erosione glenoidea.
BIBLIOGRAFIA
1. Bigliani LU, Flatow EL, Pollock RG Fratture dell'omero prossimale in La
Spalla Rockwood c.A. e F.A. Matsen Volume 1 Cap. 9, Seconda Edizione. Verduci
Editore- Roma 1999, 327-377.
2. Jakob RP, Miniaci A, Anson PS, Jaberg H, Osterwalder A, Ganz R. Four-part
valgus impaded fradures of the proximal humerus. J Bone Joint Surg Br. 1991 Mar;
73(2):295-8.
3. Neer CS 2nd. Displaced proximal humeral fractures. II. Treatment of three-part
and four-part displacement. J Bone Joint Surg Am. 1970 Sep; 52(6):1090-103.
4. Neer CS 2nd. Four-segment classification of proximal humeral fractures: purpose
and reliable use. J Shoulder Elbow Surg. 2002 Jul-Aug; 11(4):389-400.
5. Resch H, Beck E, Bayley I. Reconstrudion of the valgus- impaded humeral head
fradure. J Shoulder Elbow Surg. 1995 Mar-Apr; 4(2):73-80
Treatment of fractures of the humeral head by cemented and cementless hemiarthroplasty. Our experience
Abstract
Patients submitted to shoulder hemiarthroplasty for the
treatment of fracture of the humeral head were analyzed. The
study was conducted from 1991 to June 2001 using 2 different
prosthetic models: the Neer cemented prosthesis and the Randelli
cementless prosthesis. The authors were able to evaluate 93
cases out of 148 operated ono A review of data revealed the
essential importance of reconstruction of the tuberosity and
rehabilitation. It was also observed that the age of the patient
and the severity of the fracture did not in any way influence
results. X-ray examinations did not shed light on loosening
phenomena in prosthetic implants. Erosion of the glenoid was
observed only when two factors coexisted: incorrect position of
the prosthesis and hypomobility of the shoulder. The study
allowed us to reveal numerous prognostic elements, both
favorable and adverse, and to measure their importance and
priority.
Key words: proximal humeral fracture; hemiartroplasty;
shoulder.
Treatment of fradures of the humeral head by hemiarthroplasty
is a kind of treatment that still needs to be completely
defined. Recently, after an initial peri od of enthusiasm and optimism,
we have witnessed a criticaI analysis with subsequent decrease
in indications.
lì is the purpose of this study to contribute to the subjed,
calling attention to statistical results as well as prognostic
fadors that influence the results of treatment, so that indications for
surgery and whether or not to use the method are defined.
Material and method
The study involves patients operated on between January 1991 and
June 2001. Follow-up was 43.2 months ranging from 6 months to
10.5 years. In this period, 148 patients submitted to
hemiartroplasty. Surgery was performed on the average 4.5 days (range
2 to 18) after fradure. At the time of revision
Fig. 1
Modified Constant by decades.
Light colured columns indicate the results obtained.
53 patients had been lost to follow-up and 2 had died for unrelated reasons. We thus were able to folIow-up 93 subjects. Of these there were 74 females and 19 males. Mean age was 70.02 years. The youngest subject was 48 years old and the oldest one 91. The right shoulder was involved in 49 cases and the left one in 44. According to Neer classification 12 fractures were two-fragment, 28 fractures were three-fragment, and 53 fractures were fourfragment. The first cases (25) were submitted to surgery using the Neer cemented prosthesis. Thereafter (68 cases) the Randelli cementless prosthesis was used. For an evaluation of results we used the Constant score and the Simple Shoulder test. The mean Constant score was 62.4 (range 42 to 79), that for the SST was 6.8 (range O to 12). X-ray assessment was obtained for alI of the patients, and this allowed us to compare clinical data with that of the images.
Surgery
The patients were placed in the astronaut position. The Larghi
approach was generally used with access to the joint via
section of the tendon of the subscapularis. In cases where
severe displacement of the tuberosity was present, with upwards
movement and complete detachment of the humeral diaphysis,
access to the joint was obtained through a wide breach that had
formed saving the tendon of the subscapularis. We then proceeded
to identify and isolate the tuberosities that were entrusted
to non-resorbable wire. The humeral head was then removed
and measured in order to choose the corresponding prosthetic
head. The subsequent stage involved preparation of the humeral
diaphysis in order to carry out implant of the prosthetic
stem. Before proceeding to definitive implant amplioscopic monitoring
was always carried out with the test prosthesis and with
temporary reconstruction indicative of the tuberosity. A further
X-ray evaluation, with relative documentation of the results
obtained, was carried out after implant of the definitive
prosthesis and after accurate reconstruction, with
non-resorbable wire, of the tuberosity obtained by taking
advantage of the prosthetic holes, and, when needed, by making
holes on the humeral diaphysis. Careful passive mobilization
was always initiated as early as possible. Immobilization
in an orthosis was maintained for 4 weeks. Blood transfusions were
never necessary.
Results
The mean result for the Constant Score was 62.4 (range 42
to 79). In order to have an evaluation that is doser to reality, as
we were dealing with a series made up of patients aged an
average of 70 years, Constant must be adopted and modified based on the
different age groups (Fig. 1).
If we analyze the results for age group we see how these
are more comforting and reassuring than before. In fact, we were
able to record values that are very dose percentage-wise
to the mean value for the age group that goes from 51 to 60 years (11
patients), 84.3% for patients aged from 61 to 70 (30 cases),
88.3% for the group aged from 71 to 80 (46 patients) and
91.1% for that aged from 81 to 90 (6 patients). The 2 cases involving
patients aged 48 and 91 years were placed in the limit group
based on homogeneity (we did not want to make further subdivisions that
were not significant from a statistica l point of view).
The mean for values obtained for shoulder elevation was 112.6
degrees (values are summarized in Fig. 2). Values for
extrarotation and intrarotation are shown in Figs. 3 and
4.
As for strength the results are resumed in Fig. 5.
The results obtained for daily adivity are summarized in
Fig. 6.
The results obtained for the Simple Shoulder Test showed
a mean value of 6.8 (range O to 12).
Fig. 2
Results for elevation.
Fig. 3
Results for extrarotation.
Fig. 4
Results for intrarotation.
Fig. 5
Results for strength.
Fig. 6
Results for daily activity.
Discussion
A review of the data was carried out with the purpose of
evaluating the variables, both in terms of patient history and
surgery, that contribute to the success of surgery: age, sex,
time between fra dure and surger, approach, type of fradure,
radiotransparency, cement or no cement, glenoid erosion,
rehabilitation and patient motivation.
As may clearly be noted by looking at the T ab le in Fig. 1, age
is not an unfavorable prognostic fador; rather, as it advances,
the percentage value improves. This is naturally due to the fad
that the mean value for the Constant score (by age group) is
lowered as age rises and thus good results are more easily
achieved as well as being more realistico The modified Constant
results must, in our opinion, serve to not believe that with
older patients worse results are obtained.
Sex and time between fradure and surgery considered prognostic
elements influencing final results. There was no difference
between joint access through the subscapularis tendon or through
the breach left by displacement of the tuberosity.
Another prognostic element that we took into consideration was
type of fradure. Contrary to what we believed before the study,
we observed how type of fradure does not significantly influence
the results (Figs. 7 and 8).
Fig. 7
Fig. 8
The results were distributed
uniformly among different types of fracture with two, three
and four fragments. In fad, we observed how even a fracture with two
fragments, apparently simple to deal with surgical treatment,
can obtain less than brilliant results than a fradure with four fragments
that is considerably displaced, if the rules of good surgical reconstruction
or good functional rehabilitation are not taken into account.
A prognostic element that instead proved to be decisive in
terms of final results is that of reconstruction of the tuberosity.
Attention was paid to the position of the tuberosity during
observation and monitoring of X-rays. The site observed was compared with
Constant values: the best overall results were always associated with correct
position of the tuberosity. Not only: without the latter there were never
any satisfactory results as regards shoulder movement in elevation and in
extrarotation and in intrarotaìion (Fig. 9).
Fig. 9
The same complications (significant deficit in movement without pain) appeared when we observed resorption of the tuberosity (Fig.10).
Fig. 10
Another prognostic factor that we took into consideration
was radiotransparency. The latter, however, never related
to clinical findings. Patients, whose Xrays showed
radiotransparency, did not present any clinical signs of
pain, either spontaneous or during shoulder movement.
In none of the cases did we observe mobilization of the
prosthetic implant, in either cemented or ce me ntless implants
(Fig. 11).
Fig. 11
10.5 year follow-up
We used cemented and cementless implants. There was no
difference between the two types of prosthesis regarding
X-ray and clinical findings.
Another element that we took into consideration was erosion
of the glenoid. In our series this occurred only 3 times.
What we observed is that bone erosion occurs only when 2
factors are associated: the incorrect position of the prosthetic
head in relation to the glenoid and poor shoulder movement
(Figs. 12 and 13). In fact, when sphericity of the prosthetic
head does not coincide with the glenoid cavity, the area
in which movement takes pIace tends to narrow. When this
occurrence is associated with poor shoulder movement, the
force of attrition is concentrated in a zone that is even smaller and bone
erosion is inevitable. In cases where, instead, an incorrect position of
the prosthetic head in relation to the glenoid or very little shoulder movement
are present, we never observed bone erosion (Figs. 14 and
15).
A further element was functional
rehabilitation of the shoulder. Not always or for ali patients
was it possible to correctly carry out kinesitherapy. Patients,
often elderly and with considerable difficulty movìng around, often did
very little or no rehabilitation: in cases such as these, despite
good positioning of the implant, results for shoulder movement
provided disappointing values although the patients did not
complain of pain and despite the fact that they were subjectively satisfied.
The same may be said for patient motivation. The careful,
constant execution motivated by rehabilitation exercises always obtained
good results, while a negative attitude always produced poor results. In
conclusion, we wish to emphasize the importance of elements such as accurate
anatomical reconstruction, with particular interest in the tuberosity position,
and postoperative rehabilitation, in good results in the treatment
of proximal humeral fractures.
Fig. 12-13
Erosion of glena due to associated factors: incorrect position of prosthesis and insufficient shoulder movement.
Fig. 14
Incorrect position of prosthesis but good movement: no glenoid erosion.
Fig. 15
Poor motility but good position of prosthesis: no glenoid erosion.
REFERENCES
1. Bigliani LU, Flatow EL, Pollock RG Fratture dell'omero prossimale in La
Spalla Rockwood c.A. e F.A. Matsen Volume 1 Cap. 9, Seconda Edizione. Verduci
Editore- Roma 1999, 327-377.
2. Jakob RP, Miniaci A, Anson PS, Jaberg H, Osterwalder A, Ganz R. Four-part
valgus impaded fradures of the proximal humerus. J Bone Joint Surg Br. 1991 Mar;
73(2):295-8.
3. Neer CS 2nd. Displaced proximal humeral fractures. II. Treatment
of three-part and four-part displacement. J Bone Joint Surg Am. 1970 Sep; 52(6):1090-103.
4. Neer CS 2nd. Four-segment classification of proximal humeral
fractures: purpose and reliable use. J Shoulder Elbow Surg.
2002 Jul-Aug; 11(4):389-400.
5. Resch H, Beck E, Bayley I. Reconstrudion of the valgus-
impaded humeral head fradure. J Shoulder Elbow Surg. 1995
Mar-Apr; 4(2):73-80